| AIDScience Vol. 3, No. 11, 2003 |
| Predicting the public health impact of antiretrovirals: preventing HIV in developing countries |
| By Sally Blower1 and Paul Farmer2 |
| 1AIDS Institute and Department of Biomathematics, David Geffen School of Medicine, University of California at Los Angeles, California, United States 2Program in Infectious Disease and Social Change, Harvard Medical School, Partners In Health, Boston, Massachusetts, United States |
| Address correspondence to: [email protected] or [email protected] |
Abstract
![]() ere we discuss the potential public health impact of antiretroviral (ARV) drugs in developing countries. We use mathematical models to show that ARVs could prevent a substantial number of HIV infections, significantly reduce HIV prevalence, but would increase the transmission and prevalence of drug-resistant strains of HIV. We show that if substantial increases in risky behavior occur then antiretroviral-induced decreases in transmission will be masked. Under these conditions, HIV incidence rates will either increase or stabilize, although transmission may have been significantly reduced. We argue that ARVs should be considered as a prevention tool and not simply as a therapeutic tool; however, we stress that ARVs should be viewed as a non-conventional prevention tool since the drugs have both preventive and therapeutic effects and are given to infected, rather than uninfected, individuals.
ere we discuss the potential public health impact of antiretroviral (ARV) drugs in developing countries. We use mathematical models to show that ARVs could prevent a substantial number of HIV infections, significantly reduce HIV prevalence, but would increase the transmission and prevalence of drug-resistant strains of HIV. We show that if substantial increases in risky behavior occur then antiretroviral-induced decreases in transmission will be masked. Under these conditions, HIV incidence rates will either increase or stabilize, although transmission may have been significantly reduced. We argue that ARVs should be considered as a prevention tool and not simply as a therapeutic tool; however, we stress that ARVs should be viewed as a non-conventional prevention tool since the drugs have both preventive and therapeutic effects and are given to infected, rather than uninfected, individuals.
Recently the U.S. government has pledged to spend $15 billion in Africa and the Caribbean on AIDS prevention and care, and there has since been much debate regarding what proportion of this sum should be allocated to prevention "versus" treatment. However prevention and treatment are not mutually exclusive activities. There is ample reason to believe that prevention and care may be mutually reinforcing and overlapping activities. Here we discuss why antiretroviral (ARV) drugs should be considered as effective prevention tools, as well as therapeutic ones. Since it is widely agreed that ARVs should be used to prevent the transmission of HIV from mother to child, we will focus here on the potential impact of effective ARV therapy on AIDS control efforts in resource-poor settings. Antiretroviral usage in developing countries will provide direct and obvious therapeutic benefits for the individuals who receive treatment by increasing the length and quality of their lives. Increased availability of ARVs will also permit most patients to resume work and care for their families. However, a less obvious benefit of expanded access to ARVs in developing countries is that a high usage of ARVs could prevent a substantial number of new HIV infections (1-3), even though this expanded access will lead to substantial increases in the evolution and transmission of drug-resistant strains of HIV (1-3). Here we discuss the potential public health impact of ARVs in developing countries in terms of HIV infections prevented and reductions in prevalence. We also discuss whether treatment with ARVs should be targeted, and the potential target group that should receive ARVs.
The effect of ARVs on HIV epidemics is complex, because these therapies produce both a beneficial and a detrimental effect at the epidemic-level (1-3). ARVs reduce viral load in patients on therapy, and lower viral loads are associated with decreased rates of transmission (4), which is a beneficial epidemic-level effect. In addition, other beneficial effects can accrue. There are emerging data that improved AIDS care can enhance prevention efforts through increased uptake of voluntary counseling and testing, a cornerstone of current prevention efforts. Improved care has also led to the de-stigmatization of the disease (5, 6). As is the case with most infectious pathogens, drug-resistant strains quickly emerge under the selective pressure of ARVs. Such strains can then be transmitted (7), which is a detrimental epidemic-level effect. Mathematical models have been used as health policy tools to both quantify and predict, the epidemic-level effect of ARVs in terms of the both the beneficial and detrimental epidemic-level effects (1-3, 8, 9). Within these theoretical frameworks, drug-resistant strains emerge during treatment (due to a variety of patient, drug and treatment factors) and are transmitted. The models simultaneously track the transmission dynamics of both drug-susceptible and drug-resistant strains. The values of many of the parameters in these transmission models (for example, the fitness of drug-resistant strains relative to the fitness of drug-sensitive strains as specified by the relative transmissibility) are only imprecisely known. Therefore, generally these models of antiviral resistance have been analyzed using uncertainty analysis (10). Accurately specified point estimates of parameters are unnecessary to conduct an uncertainty analysis; only parameter ranges (i.e., upper and lower bounds) need to be defined (10). Hence, uncertainty analysis has enabled transmission models to be used as predictive tools, with the predictions presented with "uncertainty bars" (1-3). Multivariate sensitivity analyses (based upon Monte Carlo methods) have then been used to further analyze the transmission models in order to identify the key factors in decreasing transmission (1, 3), and increasing the transmission and prevalence of drug-resistance (2).
ARVs in developed countries: predicting antiretroviral resistance
To date, all of the mathematical modeling analyses of the impact of ARVs on generating antiretroviral resistance have been conducted for HIV epidemics in developed countries, where usage of ARVs has been very high. For example, the HIV epidemic in San Francisco, where 50-90% of HIV-infected individuals have received ARVs, has been extensively modeled (1-3). Both the incidence of resistance (number of cases of transmitted resistance per year) and the prevalence of resistance have been predicted for San Francisco (1, 2). Surprisingly, it has been predicted that, even with a very high usage of ARVs, transmitted resistance will initially increase and then fairly quickly stabilize at a relatively low level (Fig. 1A) (2). These modeling predictions for transmitted resistance have been compared with recently collected empirical data in San Francisco and have been shown to be correct (11). Although transmitted resistance has been predicted to remain relatively low, the prevalence of resistance (assuming a high usage of ARVs) has been predicted to rise to high levels; 42% of San Franciscans with HIV infection have been predicted to have drug-resistant virus by 2005 (Fig. 1B) (2). High levels of ARV use substantially alters the competitive dynamics between the drug-susceptible and the drug-resistant strains of HIV; the higher the usage of ARVs, the greater the reduction in the prevalence of drug-susceptible strains, but the greater the increase in the prevalence of the drug-resistant strains (Fig. 1C) (2). An analysis of these predicted data, using a model that includes both the evolution and the transmission of drug-resistant strains of HIV, has revealed that the vast majority of cases of drug-resistance that arise in a high treatment area are due to the conversion of drug-susceptible cases into drug-resistant cases during treatment (2). Therefore, in an area of high antiretroviral usage, most cases of drug resistance are due to acquired resistance, rather than to transmitted resistance. These modeling analyses show that even in developed counties (with well-developed health care systems) a high prevalence of drug-resistant HIV is to be expected.
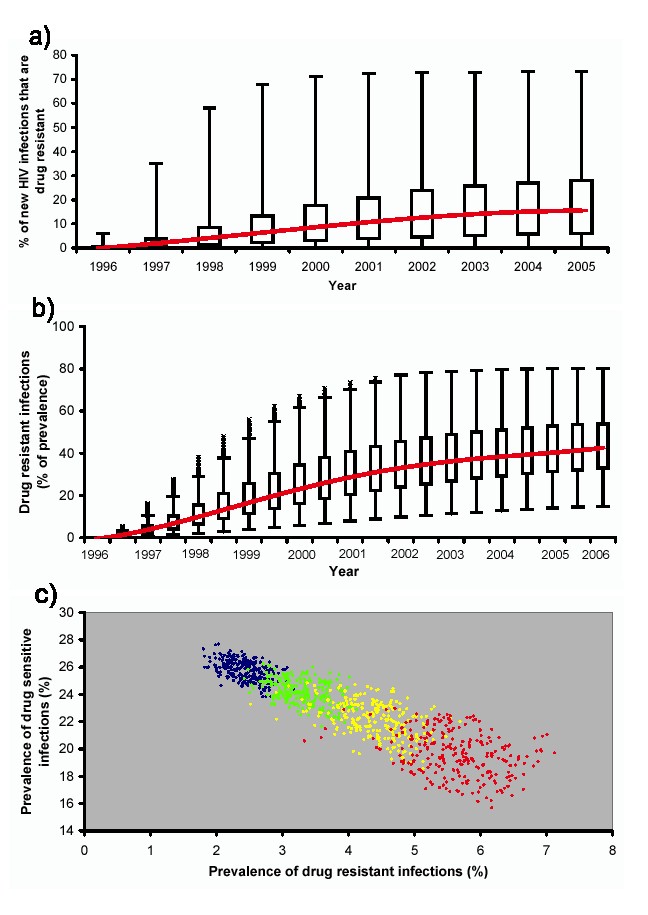 |
Figure 1. [Larger image] A) Transmission of drug-resistant HIV strains over time assuming that antiretroviral usage is high (i.e., that 50-90% of HIV-infected cases receive ARVs). Predictions made for San Francisco (2). B) Prevalence of drug-resistant HIV cases over time assuming that antiretroviral usage is high (i.e., that 50-90% of HIV-infected cases receive ARVs). Predictions made for San Francisco (1, 2). C) Increasing the proportion of HIV-infected individuals who receive ARVs alters the competitive balance between the drug-susceptible and the drug-resistant strains; blue predicted data (50-60% of HIV-infected individuals receive ARVs), green predicted data (60-70% of HIV-infected individuals receive ARVs), yellow predicted data (70-80% of HIV-infected individuals receive ARVs), red predicted data (80-90% of HIV-infected individuals receive ARVs). |
ARVs in developed countries: the impact on transmission
Mathematical models have also been used to evaluate the effect of a high rate (50-90% of HIV-infections treated) of antiretroviral usage on the overall transmission of HIV, where overall transmission is defined as the transmission of drug-susceptible strains plus the transmission of drug-resistant strains (1-3). These studies have shown that although a high usage rate of ARVs increases the transmission of drug-resistant strains, the overall transmission decreases (1-3). The decrease in the overall transmission occurs because the reduction in transmission of the drug-susceptible strains is greater than the increase in transmission of the drug-resistant strains. Thus, the modeling analyses have shown that a high usage of ARVs would result in lower incidence rates, and a substantial number of HIV infections would be averted (Fig. 2A) (1-3). Furthermore, the effect of ARVs on preventing HIV infections would increase over time (Fig. 2A). In due course, the effect of a high usage rate of ARVs decreasing incidence rates would result in HIV prevalence rates decreasing substantially over a period of a decade (Fig. 2B). The amount by which the incidence rate and the prevalence level would be reduced would directly depend upon the proportion of HIV-infected patients who receive ARVs (Fig. 2A and Fig. 2B) (1-3). Under the best of all possible conditions, mathematical modeling analyses have shown that treating a substantial fraction of HIV-infected individuals with ARVs, coupled with decreases in risky behavior, could even eventually lead to eradication of HIV epidemics, albeit in 50-100 years (3).
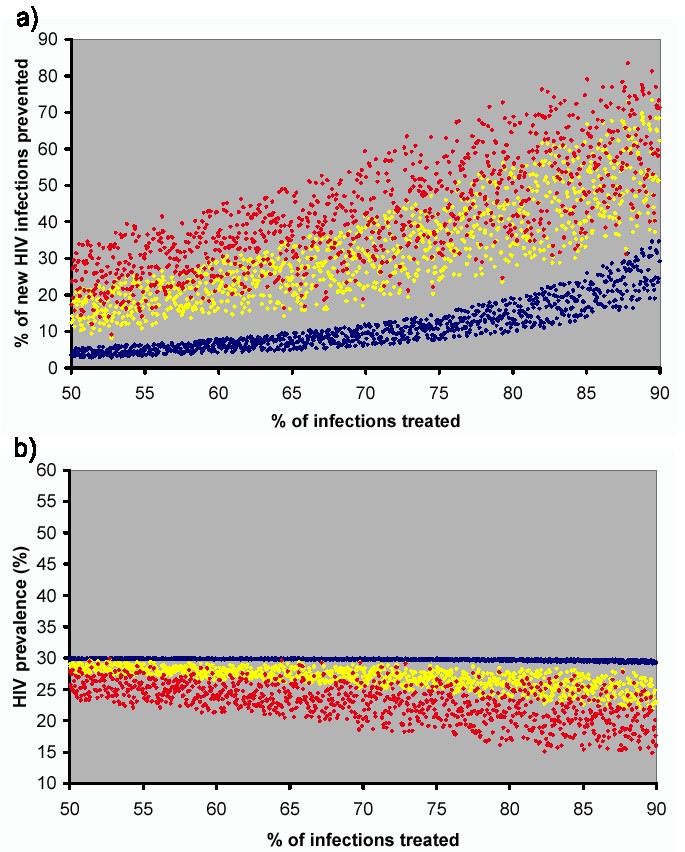 |
Figure 2. [Larger image] A) Relation among antiretroviral usage and HIV infections averted over time (assuming 50-90% of HIV-infected cases receive ARVs); using model described in references 1 and 2. Blue predicted data after one year of antiretroviral usage, yellow predicted data after five years of antiretroviral usage and red predicted data after ten years of antiretroviral usage. B) Relationship between HIV prevalence and antiretroviral usage over time (assuming 50-90% of the HIV-infected cases receive ARVs); using model described in references 1 and 2. Blue predicted data after one year of antiretroviral usage, yellow predicted data after five years of antiretroviral usage and red predicted data after ten years of antiretroviral usage. |
It is not clear whether levels of risky behavior are likely to increase in developing countries. In fact it maybe possible to decrease levels of risky behavior as increased contact between patients receiving ARVs and their health care providers provides increased opportunities for promotion of harm reduction ("secondary prevention"). However, if risky behavior increases, as is suggested by at least one study conducted within the gay community in San Francisco (12), then results from modeling analyses have shown that it may not be possible to observe antiretroviral-induced reductions in incidence and prevalence (1). Three epidemiological outcomes are possible if risky behavior increases when ARVs are made available: incidence and prevalence can 1) increase, 2) decrease, or 3) remain stable (Fig. 3A and 3B). Which of these three epidemiological outcomes will occur will depend upon the magnitude of increase in risky behavior (which will in turn depend upon the efficacy of secondary prevention messages), the proportion of HIV-infected patients on ARVs, and the degree to which these patients are rendered less infectious through viral load suppression (Fig. 3A and 3B) (1). The blue data in Fig. 3A show the balance points at which the incidence rates remain stable; at these balance points the effect of ARVs on reducing transmission equals the effect of changes in risky behavior on increasing transmission. If moderate/high levels of ARVs are used (i.e., approximately 50% of HIV-infected individuals receive ARVs) then increases in risky behavior of approximately 20% are predicted to lead to incidence rates rising (Fig. 3A) (1). Conversely, if increases in risky behavior remain below 20% the incidence rates will either decrease or stabilize (Fig. 3A) (2).
 |
Figure 3. [Larger image] A) Relation among antiretroviral usage, increases in risk behavior and HIV incidence rates after five years of antiretroviral usage; HIV incidence rates (where incidence = incidence of drug-susceptible strains plus incidence of drug-resistant strains) are plotted, blue data show the area where the HIV incidence rates are stable. B) Relationship between HIV prevalence and the magnitude of increase in risky behavior; assuming 50-90% of the HIV-infected cases receive ARVs; using model described in references 1 and 2. Blue predicted data after one year of antiretroviral usage, yellow predicted data after five years of antiretroviral usage and red predicted data after ten years of antiretroviral usage. |
Evidence from Brazil, the only developing country with a comprehensive AIDS prevention-and-care program with a high proportion of patients on ARVs, suggests that use of these drugs has already led to a decline in incidence in this country. Epidemiological surveillance data released in 2002 shows that HIV incidence has declined in recent years now that ARVs are widely available — only 7,361 new cases of HIV disease were registered in the first nine months of 2001, compared to the 17,504 cases registered in 2000 (13). Furthermore, widespread antiretroviral use has reduced hospitalizations and led to a substantial reduction in tuberculosis incidence. The Brazilian Ministry of Health estimates that cost savings for reduced hospital admissions and treatment of opportunistic infections between 1997 and 2001 have been close to $1.1 billion (14). Projections based upon modeling made in the early nineties have been proven incorrect, as Brazil’s HIV epidemic has contracted rather than expanded.
ARVs in developing countries: the impact on transmission
The modeling analyses that have been done so far have been to predict the impact that ARVs have had (and will have) in developed countries, where a high proportion of HIV-infected individuals receive ARVs. These analyses have predicted that a high usage of ARVs can substantially decrease the overall transmission rate, and therefore that providing ARVs should also be viewed as an effective public health prevention strategy, as well as an effective therapeutic strategy (1-3). The potential impact of ARVs in developing countries is less clear as the proportion of HIV-infected individuals who will receive ARVs will be considerably less than in developed countries. Currently, it is estimated that less than 1% of HIV-infected individuals in the most heavily burdened developing countries receive effective ARV therapy. It has been calculated that, if 25% of infected individuals in South Africa received ARVs, 19% of projected new HIV infections would be prevented over a five-year period (15). However, this calculation is based upon the optimistic assumption that drug-resistant HIV will not arise. If it were assumed that drug-resistant HIV can arise and be transmitted then 50% of the HIV-infected individuals would have to receive ARVs in order to avert 10-30% of new HIV infections over the next decade (Fig. 1A). However, any magnitude of reduction in new HIV infections in developing countries is substantial when viewed in terms of absolute numbers of lives saved, as incidence rates in many developing countries are extremely high. However, it should be noted that it may not be possible to observe antiretroviral-induced reductions in the incidence rates, because if substantial increases in risky behavior occur then the antiretroviral-induced decreases in transmission will be masked (Fig. 2A) (1). Under these conditions, although transmission will have been reduced, the HIV incidence rate will either increase or stabilize (Fig. 2A) (1); therefore, although ARVs could serve as a fairly effective prevention strategy in developing countries the magnitude of the prevention effect will be substantially underestimated if it is only evaluated by measuring incidence rates.
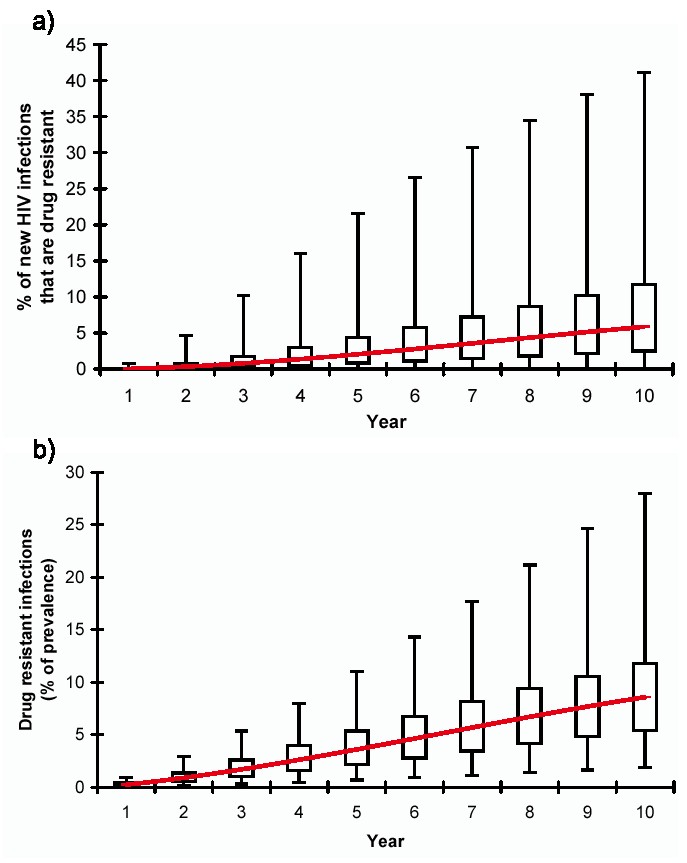 |
Figure 4. [Larger image] A) Transmission of drug-resistant HIV strains over time in a developing country assuming that antiretroviral usage is moderately high (i.e., median 30% of HIV-infected cases receive ARVs). Red line shows median values. B) Prevalence of drug-resistant HIV cases over time in a developing country assuming that antiretroviral usage is moderately high (i.e., median 30% of HIV-infected cases receive ARVs). Red line shows median values. |
As in developed countries, increasing access to ARVs in developing countries will prevent HIV infections, but will increase levels of drug-resistant viruses (1, 2). If 30% (median value) of the HIV-infected individuals in developing countries receive ARVs, then (after 10 years) the prevalence of drug resistance can be expected to be 9% (median value) of prevalent infections, with a possible maximum value of 28% (Fig. 4). Thus, if ARVs are to be viewed as prevention tools careful thought must be given to designing epidemic-control strategies that balance the conflicting public health goals of reducing 1) overall transmission and 2) the emergence and transmission of drug-resistant HIV. Health policy planners will need to decide what are the appropriate public health goals for antiretroviral usage in terms of defining what is the "acceptable balance" between preventing infections and increasing the burden of drug-resistant strains. Specifically, public health policy officials will have to grapple with two questions: "How much drug-resistant HIV is acceptable?" and, of even greater importance, "How many deaths from pan-susceptible HIV are acceptable?" It is estimated that AIDS will kill three million people during 2003, and the vast majority of them will die of pan-susceptible HIV.
Antiretrovirals: an unconventional HIV prevention tool
ARVs should be considered as a prevention tool as they reduce the transmission rate, but they should not be used in exactly the same manner as conventional prevention tools for sexually transmitted diseases (STDs). Conventional prevention tools for STDs (such as condoms or educational interventions) are generally targeted at uninfected individuals who are part of behavioral core groups, e.g., sex workers. Behavioral core groups are relatively small in size, but because of their high level of risky activity disproportionally contribute to transmission. Hence conventional prevention strategies targeted at behavioral core groups have the potential to have a substantial effect on reducing the transmission of HIV (or other STDs). A targeted prevention strategy using conventional prevention tools directly benefits the uninfected individuals in the behavioral core-groups, but does not lead to any "loss of benefit" to the uninfected individuals outside of the behavioral core groups. However, we argue that ARVs should be viewed as a non-conventional prevention tool because the drugs have both preventive and therapeutic effects and are given to infected (rather than uninfected) individuals.
ARVs have at least two benefits: they provide a potential preventive benefit to all of the uninfected individuals in the community, but they provide a direct therapeutic benefit only to the HIV-infected individuals receiving the treatment. The children of young adults whose lives are prolonged by ARVs may also be considered direct beneficiaries, since in poorer countries maternal death is associated with decreased child survival. An epidemic-control strategy that utilizes ARVs simply as a conventional prevention tool and targets behavioral core groups is an explicit decision to provide therapeutic benefit preferentially to the core-groups; thus the non-core group suffers a substantial loss from such a targeted "prevention" strategy as they do not receive any therapeutic benefits. Hence targeting ARVs to behavioral core groups would be unethical and totally impractical. It would be impossible to identify members of the actual behavioral core group, as all HIV-infected individuals would claim to be in the behavioral core group in order to be eligible for treatment. Also, a treatment targeted to a behavioral core group rather than mass treatment could be epidemiologically unsound and lead to significantly higher levels of drug resistance and increased transmission rates. If targeted treatment needs to be considered due to limited resources then an alternative strategy would be to target the sickest AIDS patients, as has been done in Haiti (5). It may be assumed that these patients will have the highest viral loads, and therefore that targeted usage of ARVs in this subset would be the strategy that would optimize both therapeutic and preventive goals. Such a strategy would be epidemiologically sound, as well as ethical and practical.
Predicting the future
To date the only beneficial effects of ARVs that have been included in the modeling analyses have been the effects of ARVs on reducing transmission. There are many additional benefits of increasing usage of antiretroviral usage that should be included in future modeling analyses so that the complete benefits of ARVs as prevention tools in developing countries can be quantitatively assessed. It is increasingly clear that better HIV care, which necessarily includes ARVs, can increase interest in voluntary counseling and testing, lessen AIDS-related stigma and decrease the high drop out documented among health care workers in the most heavily burdened areas. Furthermore, good HIV care means that patients living with HIV have more regular and more satisfactory contact with health care workers, affording the latter the chance to reinforce secondary prevention messages and harm-reduction strategies. Good HIV care in those countries most heavily burdened with AIDS deaths may also reduce the demoralization among health care providers that, though well known by all who work in such settings, is only now being assessed as a major cause of "brain drain" and burn out (16). Mathematical modelers need to move beyond transmission models and traditional economic analyses in order to model the full biosocial complexity of the HIV epidemic and to assess the full impact of ARVs in developing countries.
In developing countries, as in developed countries, the epidemic-level impact of ARV usage will depend critically upon how widely treatment is made available, and how well it is used. The effect of ARV usage on HIV epidemics is complex. Both the beneficial and the detrimental impacts on the epidemic will depend on the proportion of HIV-infected individuals who receive ARVs. Currently, in the poorest and most heavily burdened countries, almost no HIV-infected individuals are receiving ARVs in an effective manner. If only a small fraction of HIV-infected individuals receive ARVs, there will be almost no impact on transmission, and only low levels of drug-resistant HIV will arise. In developing countries where antiretroviral usage reaches moderately high levels, ARVs will decrease transmission, but fairly high levels of drug resistant HIV can be expected. Treatment can act as a prevention tool, but it is an unconventional prevention tool as it is given to the HIV-infected individual rather than to the uninfected individual. Health policy decisions should be made on the basis that ARVs are first and foremost a therapeutic tool, and the effects of ARVs as a prevention tool are secondary. When designing epidemic-control policies for developing countries, the impact of ARVs on preventing transmission should be evaluated, but any decisions on allocation of treatment should be ethical as well as practical and epidemiologically sound. Such debates should also seek to incorporate the full biosocial complexity of the modern AIDS epidemic rather than further reinforce rigid distinctions between HIV prevention and care. ARVs are already available for less than a dollar per day, and they will be widely used throughout the poorest parts of the world. The degree to which such agents will be used wisely and widely will depend to no small extent on policymakers’ ability to move beyond sterile debates. It is essential that access to well-controlled use of ARVs be increased in developing countries. Substantially increased access is likely to significantly reduce both the mortality and the overall transmission of HIV.
References and notes
| 1. | S. M. Blower, H. B. Gershengorn, R. M. Grant, Science 287, 650 (2000). PubMed |
| 2. | S. M. Blower, A. N. Aschenbach, H. B. Gershengorn, J. O. Kahn, Nat. Med. 7, 1016 (2001). PubMed |
| 3. | J. X. Velasco-Hernandez, H. B. Gershengorn, S. M. Blower, Lancet Infect. Dis. 2, 487 (2002). PubMed |
| 4. | T.C. Quinn, et al., N. Engl. J. Med. 342, 921 (2000). PubMed |
| 5. | P. Farmer, et al., Lancet 358, 404 (2001). |
| 6. | P. Farmer, et al., Bull. World Health Organ. 79, 1145 (2001). PubMed |
| 7. | S. J. Little, et al., N. Engl. J. Med. 347, 385 (2002). PubMed |
| 8. | E. Tchetgen, E. H. Kaplan, G. H. Friedland, J. Acquir. Immune Defic. Syndr. 118, 118 (2001). PubMed |
| 9. | J. Goudsmit, AIDS 15, 2293 (2001). PubMed |
| 10. | S. M. Blower, H. Dowlatabadi, Int. Stat. Rev. 2, 229 (1994). |
| 11. | S. M. Blower, A. N. Aschenbach, J. O. Kahn, Lancet Infect. Dis. 3, 10 (2003). |
| 12. | M. H. Katz, et al., Am. J. Public Health 92, 388 (2002). PubMed |
| 13. | Brazilian epidemiological data, Boletim Epidemiológico — AIDS [online] XV(1). Available online |
| 14. | Brazilian Ministry of Health. National AIDS Drug Policy. Brasília: Coordenação Nacional de DST e AIDS, Ministério de Saúde (2002). |
| 15. | E. Wood, et al., Lancet 355, 9221 (2000). Available online |
| 16. | G. Raviola, M. Machoki, E. Mwaikambo, M. J. Good, Cult. Med. Psychiatry 26, 55 (2002). PubMed |
| 17. | Sally Blower acknowledges the financial support of NIH/NIAID grant RO1 AI41935. We are very grateful to Nick Aschenbach and Li Ma for constructing the figures for this perspective. We also thank Nicole Gastineau for her help in making this perspective possible. |
| Copyright © 2001 by The American Association for the Advancement of Science |